

Introduction
Red blood Cell (RBC) transfusion therapy is an important disease modifying treatment in sickle cell disease (SCD). RBC alloimmunization is one of the more serious complications associated with transfusion therapy and limits its wider clinical application. This complication can result in both acute and delayed hemolytic reaction in the recipients. It is unknown at this time if alloimmunization can lead to broader downstream end-organ complications in sickle cell disease.
In this retrospective study, we analyzed the complications associated with RBC alloimmunization in the Central Missouri SCD cohort following development of allo- antibodies (Allo-Ab).
Methods
We performed a retrospective chart review of all SCD individuals treated at the University of Missouri Medical Center from December 2000 to 2017. Only SCD patients that received RBC transfusions at the Center were included in the study. A two-tailed student's t-test was used to analyze all continuous variables. Fischer's exact test was used to analyze all categorical variables. Apvalue of <0.05 was considered statistically significant.
Results
Of the 130 SCD patients, 80 patients were eligible to be included in the study based on available laboratory and clinical data. There were 51 HbSS, 25 HbSC, and 4 HbSβ0/+ patients, and overall, 28% of the patients had alloantibodies following transfusion therapy.
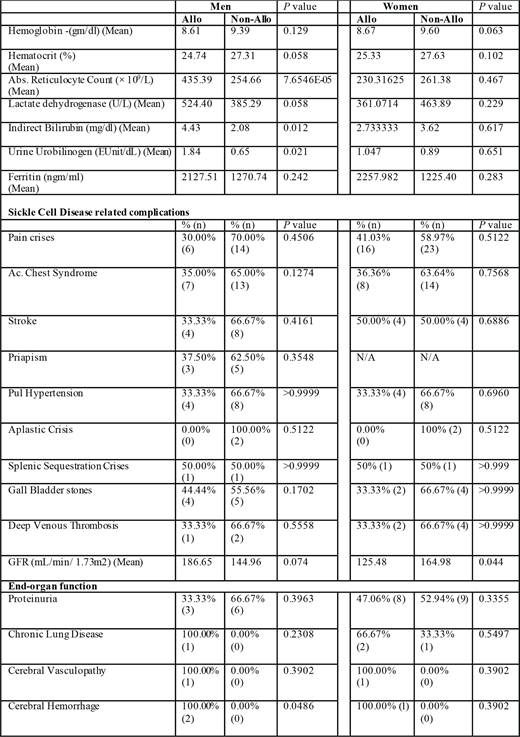
The mean hemoglobin and hematocrit were lower in alloimmunized versus non-alloimmunized (8.65 gm/dl vs 9.48 gm/dl, p = 0.016) SCD individuals. Reticulocyte count, total bilirubin (2.9 mg/dl versus 1.8 mg/d, p = 0.02), and urine urobilinogen were elevated in allo-immunized individuals. Overall, alloimmunized patients received more packed red blood cell (PRBC) units/life year (9.18 versus 3.60 units, p = 0.021). Demographic factors like age of first transfusion, systolic, diastolic, and mean blood pressures were not significantly different between the groups. Inflammatory markers such as erythrocyte sedimentation rate (ESR) and C- reactive protein (CRP) were not significantly different in alloimmunized and non-alloimmunized individuals. Absolute neutrophil count, platelet count, and lymphocyte counts were not significantly altered in patients with and without allo-AB. Hemoglobin F concentration or hydroxyurea usage were not significantly different between the groups.
Distinct gender differences in hematological profile and end-organ complications were observed in allo-immunized individuals (Table 1). Indirect markers of hemolysis were persistently elevated in alloimmunized men (Table1) compared to women. Seizures were an associated complication in alloimmunized compared to non-alloimmunized (66.6% versus 33.3%, p = 0.0058) men. Decreased glomerular filtration rate (GFR) was observed in women with alloimmunization compared to men.
Conclusions
Alloimmunization in men is associated with distinct downstream complications compared to women. Persistence of elevated indirect markers of hemolysis were observed more in men with allo-Ab. Men with allo- Ab had more central nervous system complications compared to women. These findings have important clinical and therapeutic significance and needs to be tested in larger clinical trials.
Busken:ASH:Other: 2018 HONORS Award Recipient.

